

By Victoria Strang
During my junior year of college, I traveled to South Africa as part of a student group examining international and community-based health efforts. It was the spring of 2009, and the HIV/AIDS epidemic continued to plague the country. Stigma surrounding the disease was heightened due to the government’s denial of its spread and a lack of education on paths of transmission. While health clinics and education centers were working hard within the vast shanty towns on the edge of the city, the continued shame surrounding a diagnosis of HIV led many to forgo treatment or seek out education around prevention. After getting accustomed to the whispered voices and hushed tones used when speaking about HIV/AIDS, I was surprised one day to see a man walking down the middle of the street wearing jeans and a white t-shirt that read, “I AM HIV-POSITIVE.”
I soon discovered that this man was the pastor of a local church whose small metal structure complete with 20 plastic lawn chairs had become one of the few places in the town where one could speak openly about the disease that was killing hundreds of thousands of South Africans each year. I began to follow the pastor as he visited HIV-positive individuals and their families, and after talking with several of his congregants I gained the courage to ask them about the pastors own HIV status. The man quickly replied, “No, the pastor does not have HIV but if people in his congregation have HIV, he has HIV.” It was through this experience that I first understood the power of religion in the work of public health.
Through my own work in organizing faith communities around issues of social justice I have found that many people do not associate the Gospel with public health. And yet, nearly one-fifth of the Gospel is dedicated to Jesus’s healing ministry. Health’s centrality in the Gospel is further emphasized by the work of the disciples to whom Jesus grants, “the authority over unclean spirits, to cast them out, and to cure every disease and every sickness” (Matthew 10). Throughout the Acts of the Apostles we read about the disciples’ own travels spreading the Gospel and healing those who are crippled or paralyzed. However, for all its prominence in the Gospel text, the call of healing is not one taken up by many congregations today. While the enlightenment may have altered our understanding of healing from one centered in the miraculous to one based in biological medicine, that does not mean that individual Christians and churches no longer have a role to play in the health of their community.

During the time of Jesus’ ministry being crippled, blind, or showing signs of disease could not only be physically painful but socially isolating. The promise of health meant that one could regain social, economic, and religious standing not only for oneself but for ones family. Jesus’ ability to heal meant much more than the mere alleviation of physical suffering – it was an equalizer. While we may have a better understanding of the root cause of disease and improved treatment measures in the 21st century, disability and illness can still illicit social stigma as well as prevent individuals and families from gaining economic stability. Many Americans struggle to pay their medical bills even if they have insurance. The high cost of care can lead individuals to delay medical treatment ultimately leading to more serious, and costly medical interventions. Families have reported taking money from retirement or college savings accounts and in some scenarios even filing for bankruptcy. It is no secret that the U.S. spends the most of any developed country on health care (roughly 17.4% of our GDP) yet we still fall behind in meeting the health needs of our citizens. Having recently worked on a project examining maternal mortality and morbidity in Georgia I was shocked to learn that the number of women in the U.S. dying in pregnancy and childbirth is on par with countries such as Iran, Libya, and Turkey. The cost of care coupled with a lack of health education and continually diminishing resources has perpetuated a cycle of ill health impacting our nation and its most vulnerable populations.
The reason why I have chosen to work with communities of faith around access and education for health is not simply due to my own religious beliefs, but because pragmatically faith groups serve as one of the last vestiges of organized community. While the number of practicing Christians may be declining, churches represent a unified structure that can motivate and mobilize people. We should not ignore the power of a group of like minded individuals who share a core moral understanding that we are called to assist those who have been marginalized by society.
Public health is one of the most pressing issues of out time and communities of faith can work towards a right vision of health in two ways.
First, they can lend their voice to political discussions around health education and access to services on both a state and national level. Groups such as Faith in Public Life, PICO, and NETWORK have done this through advocacy initiatives involving lobby days, legislative endorsements, and other forms of political mobilization.
Second, faith communities can serve as a resource for people seeking health information, services, and other resources. Research has shown that in traditionally marginalized communities the involvement of local churches in health programs can greatly impact health outcomes. Therefore, churches could host educational events on illnesses effecting congregation and community members such as diabetes and heart disease; hold weekly exercise classes and/or meeting groups; or direct care services for pregnant women, those living with HIV/AIDS and other illnesses. Churches can also partner with national organizations such as The American Heart Association and Planned Parenthood or with local hospitals to host health fairs. In so doing, pastors, deacons and lay leaders can help build trust between their congregants and public health administrators. This is particularly important in populations that have historically been abused by the medical profession or fear legal repercussions due to immigration status.
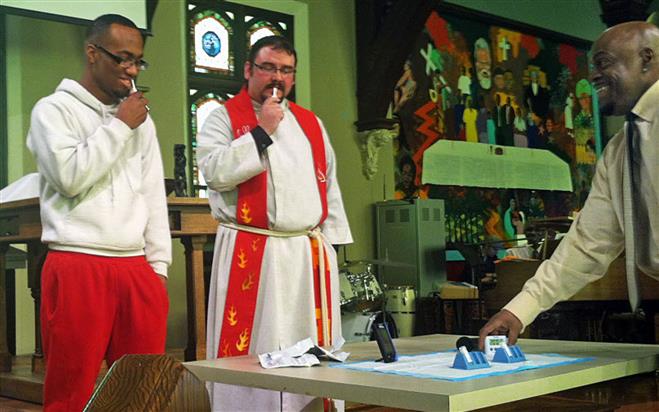
Additionally, religious leaders can help reduce stigma around disease and disability. With the recent growth of HIV/AIDS cases in the American South, pastors and denominational bodies have partnered with community health centers and local nonprofits to educate their congregations about sexual health as well as provide financial and emotional resources to those who are infected. Additionally, a number of pastors have helped alleviate social stigma by speaking about HIV/AIDS during sermons and getting tested in front of their congregations during worship services. Religious leaders have an important role to play not only in the education and protection of their congregants but to work towards improving the health of the wider community. This includes collaborating with hospitals, community healthy clinics, and nonprofits on ways to reach underserved populations and empower them with the tools and resources needed to live a fully and healthy life.
Growing up in the United Church of Christ, I was drawn to the figure of Jesus through his emphasis on social justice and the elimination of social and structural inequalities. While I did not have the Biblical foundation the for the type of social justice work I wanted to do when I entered, in my graduate theology work at Yale, I have recognized the power of the Gospel when thinking about how Christians can organize around the issue of health care. Community organizing can be a powerful tool for change. We have seen this not only in our country’s history but in recent responses to the new political administration. Jesus was the original community organizer, seen throughout his ministry and in his call to the disciples to spread a vision of equality. At the center of this vision was the promise of health. In a country that continues to view health care as a commodity rather than a right, we are negating the Biblical mandate set out by Christ. In looking to the Gospel we see that Christians are called to speak up and spread the ministry started by Jesus to promote health in our own communities and in our nation.
Resources:
- Health Care Law & Your Community: Key Information for Faith and Community Leaders (pdf through the Center for Faith-based and Neighborhood Partnerships)
- National Heart, Lung, and Blood Institute Faith-Based Toolkit
- Faith Based Cancer Disparities Initiative Resource Toolkit (pdf)
- National Diabetes Education Program: Resources for Faith Leaders and Health Ministers (pdf)
- HIV/AIDS Ministry Archdiocese of Atlanta
- Let’s Move Faith and Communities (pdf through the U.S. Department of Health and Human Services)
- Many state health departments and local nonprofits also provide outreach toolkits through their websites.
Victoria Strang is a Master of Divinity Student at Yale University where she studies the integration of faith-based programing into public health initiatives. Prior to Yale, she served as the Strategic Initiatives Manager of the Faith Outreach program at the Humane Society of the United States where she worked with religious leaders across the country on environmental issues related to food production and animal welfare. She currently consults with several public health organizations on faith-based outreach and educational programs.
Image sources:
(1) https://lifehopeandtruth.com/bible/is-the-bible-true/how-do-we-know-the-bible-is-true/health-science-and-the-bible/
(2) http://archive.jsonline.com/news/opinion/pastors-hiv-test-shines-light-688v1gj-195452601.html
(3) http://www.ucc.org/justice_health

You must be logged in to post a comment.